Abdomen
Visceral Organs
THE KIDNEYS
Location and External Anatomy
The left and right kidneys lie in the retroperitoneal space on either side of the spine in the superior lumbar region of the posterior abdominal wall. The roughly fist sized organs are protected by the 11th and 12th ribs as well as muscle and fat tissue. They lie in the T12-L3 region, with the right kidney lying slightly lower due to displacement from the liver. The kidney’s unique shape includes the convex lateral side and a concave medial surface containing a vertical cleft called the hilum. The hilum is a small area for the renal artery and nerves to enter the kidney, and for the renal vein and ureter to exit. Lying atop the kidneys, on both sides, are the adrenal glands, which serve an endocrine function in the body and don’t relate functionally to the kidneys.
Gross Anatomy
The Kidney is composed of 2 regions, namely, the outer renal cortex and the inner renal medulla. The cortex is light and has a granular appearance. The darker renal medulla contains cone shaped structures called renal pyramids, which are separated by renal columns that project inward from the renal cortex. Each section of renal pyramid and its surrounding renal columns are called the lobes of the kidney. Every kidney can have a range of 5 to 11 lobes each. The renal pelvis, which is the broadened superior portion of the ureter, branches into major calices and then further into minor calices. Minor calices are cup-shaped tubes that enclose the papillae of the renal pyramids. In this location, the papillae drain urine from the pyramids into the calices, which then empty into the renal pelvis.
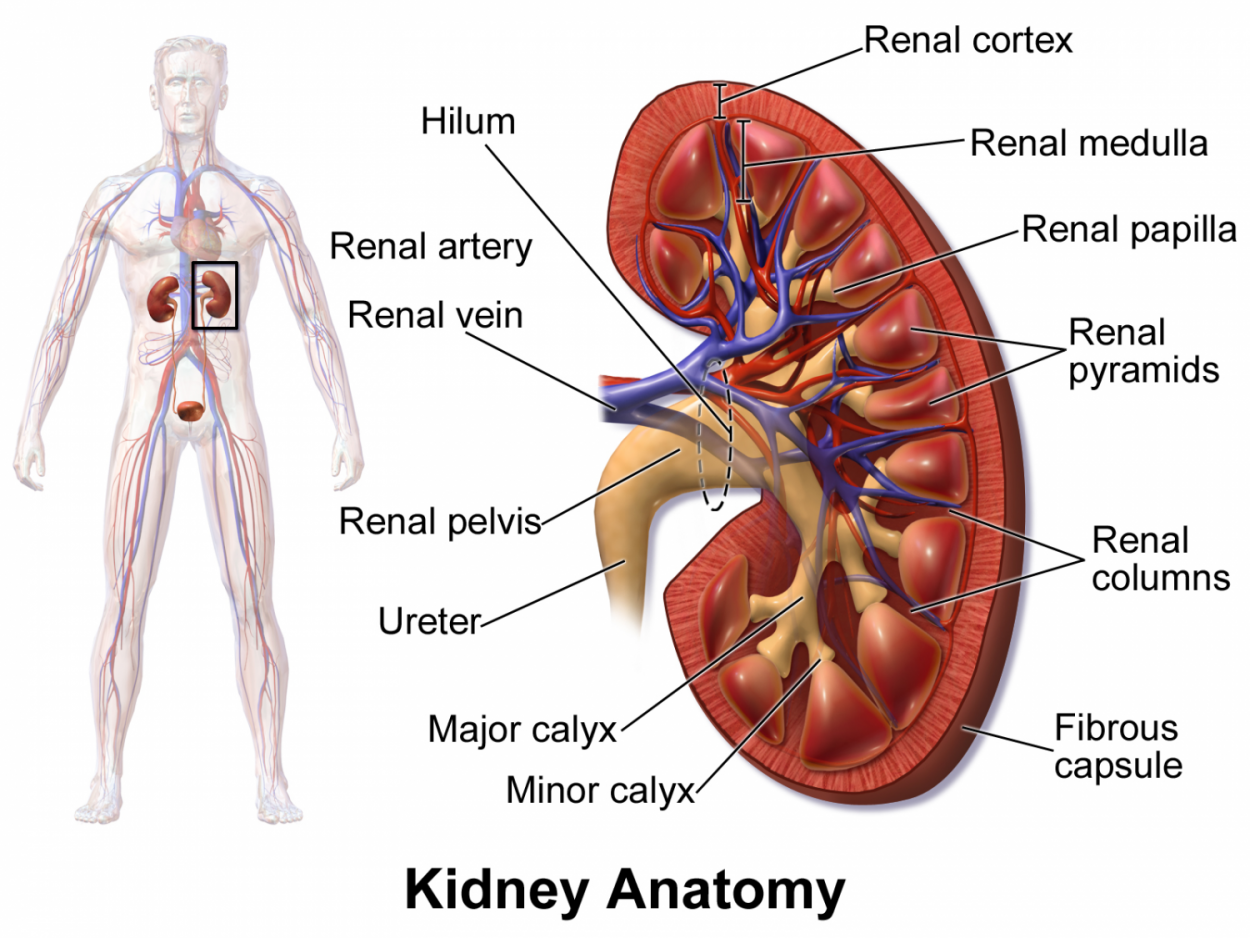
Figure 1.0. Anterior frontal section diagram of the gross anatomy and blood supply of the right kidney.
Nerve and Blood Supply
Because of the kidney’s function in cleansing the blood, they require a rich supply of blood. During rest the kidneys receive about one quarter of the heart’s systemic output via the renal arteries. The renal arteries branch off of the abdominal aorta at right angles between the 1st and 2nd lumbar vertebrae. When they reach the hilum of the kidney they branch off into five segmental arteries. Once they enter the renal sinuses they divide even further into the interlobar arteries. These arteries lie in the renal columns between each renal pyramid. As they turn the corner over the bases of the renal pyramids they transform into arcuate arteries where the cortical radiate arteries project outward into the cortical tissue. Further, the cortical radiate arteries reach the glomerular capsule via the afferent arteriole then to the efferent arteriole and out to the peritubular capillaries. The blood now exits the nephron into the cortical radiate vein, arcuate vein, interlobar vein, and out the kidney through the renal vein into the inferior vena cava.
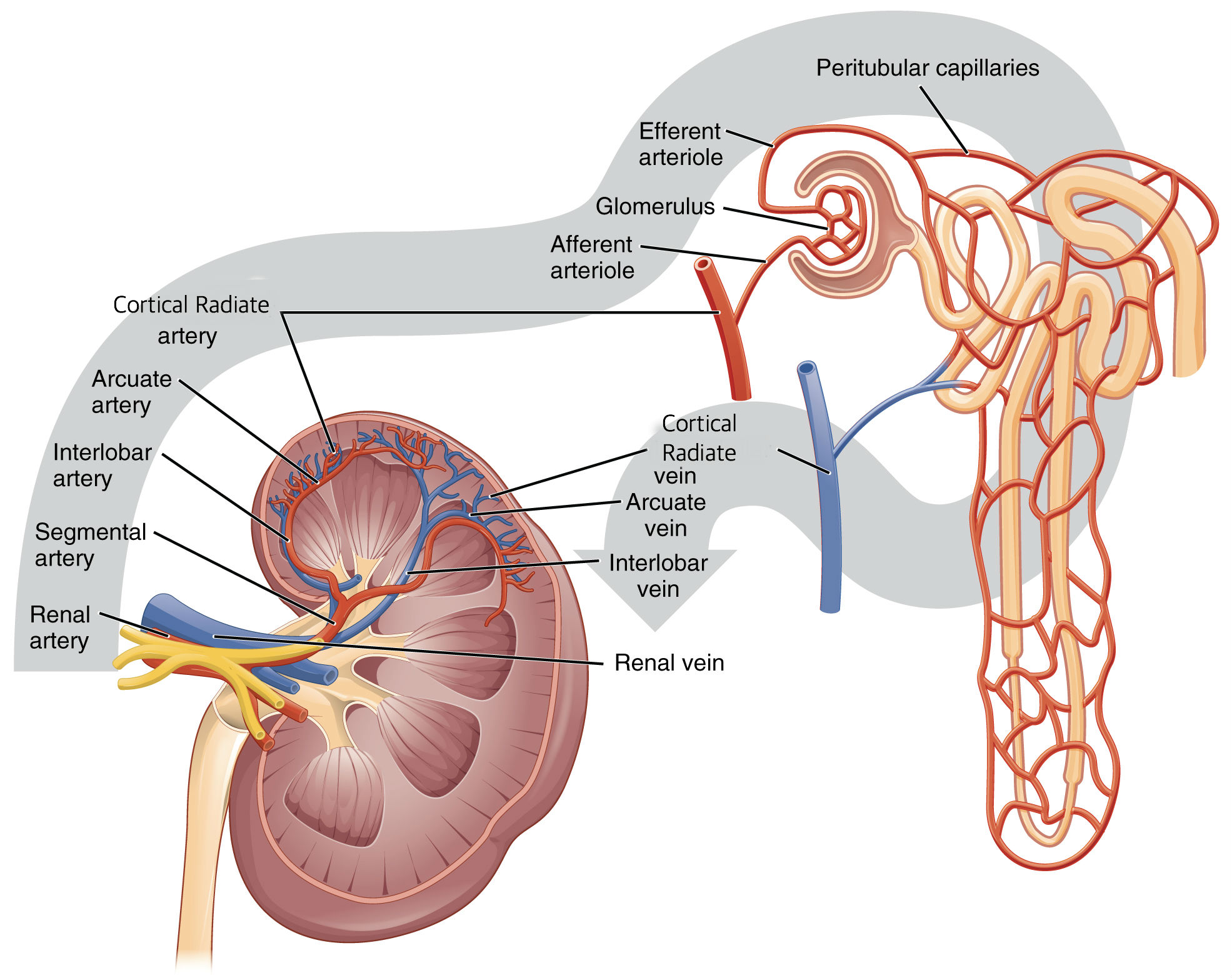
Figure 2.0. Illustration of the path of blood flow entering and exiting the kidney.
Microscopic Anatomy
The most important structural and functional portion of the kidney is the nephron. Inside each kidney there are about one million nephron tubules packed together. The nephron is so important because it produces urine through filtration, resorption, and secretion. A nephron is composed of 2 structures: the renal corpuscle and the renal tubule. Inside the renal corpuscle, which lies in the renal cortex, there is a glomerulus (a tuft of capillaries) and a glomerular capsule surrounding it. The glomerulus is where filtration occurs. Once the fluid has been filtered in the glomerulus it leaves and enters the renal tubule. The renal tubule consists of the proximal convoluted tubule, the nephron loop (Loop of Henle), the distal convoluted tubule, and the collecting ducts. Throughout the tubules tubular resorption occurs. Tubular resorption is the return of water and solutes that were filtered from the blood at the renal corpuscle back into the blood. This process occurs through active transport, facilitated diffusion, symport, and osmosis. The structure of the tubules allows for increased time and surface area for processing the filtrate. The processed urine then enters the collecting ducts where they eventually drain into the minor calices and out to the ureters.
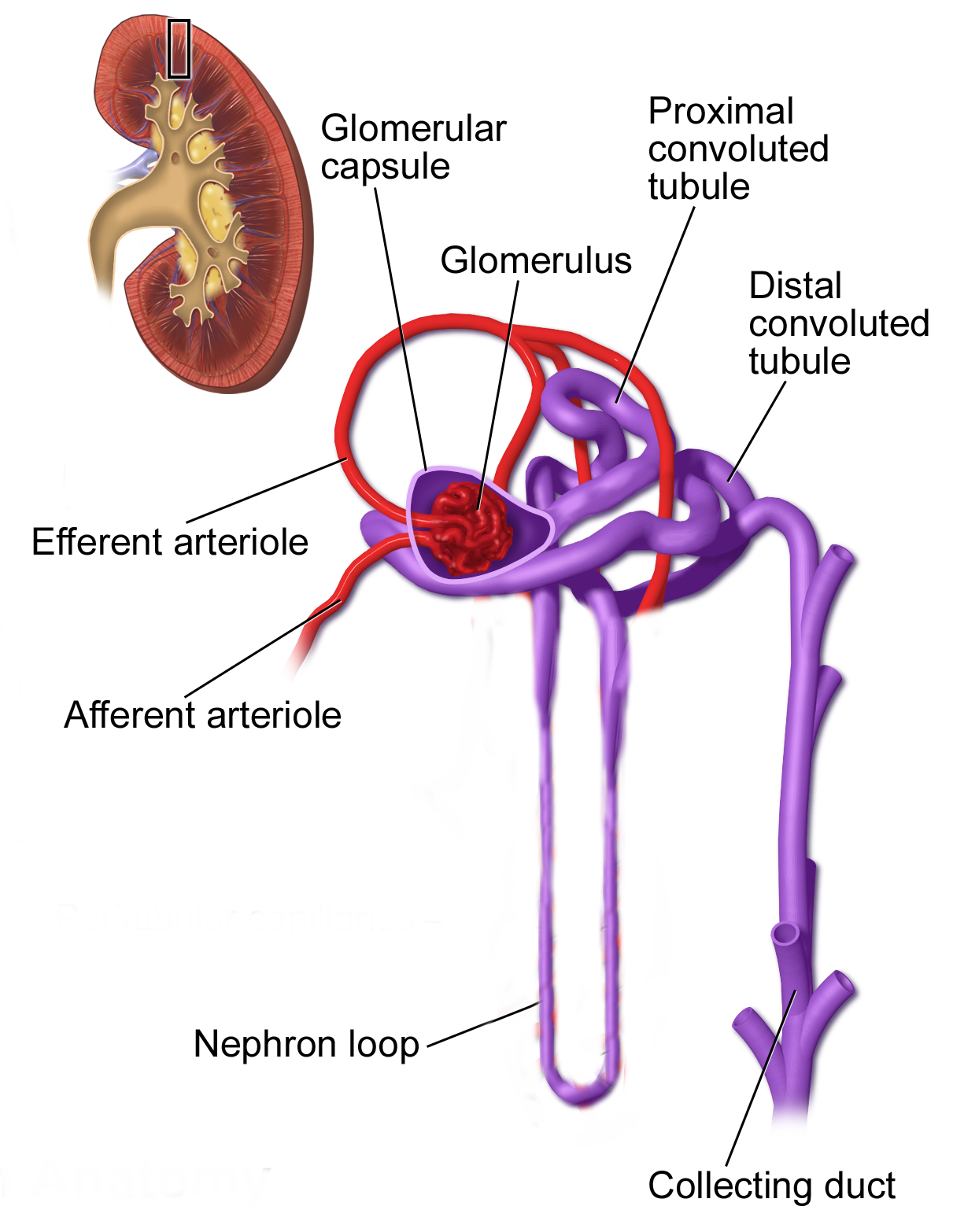
Figure 3.0. Illustration of the structural characteristics of a nephron. The vasculature surrounding the nephron loop has been removed for optimal viewing.
THE URETERS
Gross Anatomy
The structures that follows the kidneys in the urinary tract are called the ureters. The ureters are 10 inch long tubes that leave the kidney through the hilum and transport urine to the urinary bladder. They descend retroperitoneal (behind the peritoneum) through the abdominal cavity and across the sacroiliac joint, where they then enter the posterolateral corner of the urinary bladder obliquely. This oblique or angled entrance into the bladder prevent backflow of urine back into the ureters.
Microscopic Anatomy
The walls of the ureters consist of 3 tissue layers called the mucosa, the muscularis, and the adventitia. The mucosa layer is made of transitional epithelium, which has the ability to stretch when urine fills the ureters, and a lamina propria containing fibroelastic connective tissue for more support. This layer also contains goblet cells that secrete protective mucous. The middle tissue, called the muscularis, consists of 2 layers: an inner longitudinal layer and an outer layer of circular smooth muscle. In the inferior third of the ureter is a 3rd muscularis layer that helps with peristalsis of urine. Peristalsis is stimulated in the muscularis layer when urine passes through the ureters, propelling urine down to the bladder in waves. The outer tissue of the ureter wall is the adventitia composed of typical connective tissue.
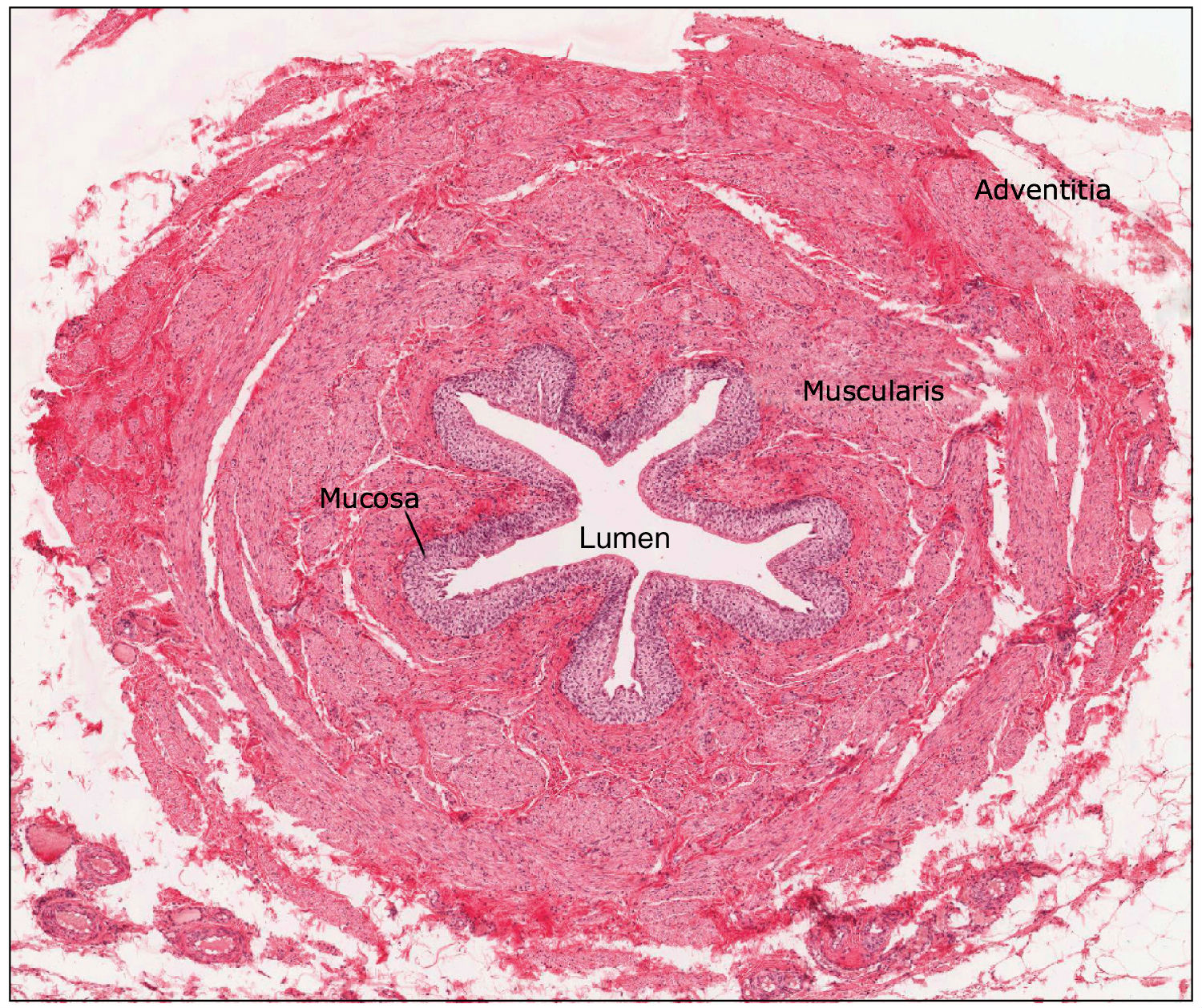 Figure 4.0. The 3 tissue layers of the ureter function as protection, movement of urine (peristalsis) and structure.
Figure 4.0. The 3 tissue layers of the ureter function as protection, movement of urine (peristalsis) and structure.
THE URINARY BLADDER
Location in the Body
The urinary bladder is a muscular sac that stores and expels urine out of the body. It lies inferior to the peritoneal cavity on the pelvic floor and is directly posterior to the pubic symphysis of the coxal bone. There are slight differences in males and females in the location of the bladder. In females the bladder lies anterior to the uterus, vagina, and rectum. In males the bladder lies anterior to the rectum and the prostate gland lies directly inferior.
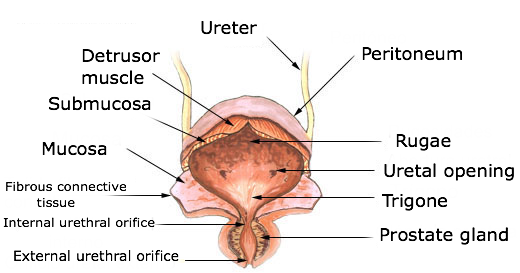 Figure 5.0. Labelled diagram of the urinary bladder, ureters, and urethra of a female.
Figure 5.0. Labelled diagram of the urinary bladder, ureters, and urethra of a female.
Gross Anatomy
The shape of the bladder depends on whether or not it is empty or full. A full bladder is roughly spherical and as it gets more full it pushes superiorly into the abdominal cavity. In contrast, an empty bladder has the shape of an upside down pyramid, with 4 corners and triangular surfaces. The posterolateral surface, again, is where the ureters enter the bladder obliquely. The anterior angle (apex) is made of a fibrous band called the urachus. Urachus means “urinary canal of the fetus” and is a closed part of what used to be an embryonic tube called the allantois. The inferior angle, also called the neck, is the area that drains urine from the bladder and into the urethra for excretion. A significant area inside the urinary bladder, called the trigone, is where the openings for both ureters and the urethra form a triangular area. This area is important clinically as it is a common site of infection persistence. Conditions related to the urinary tract are further described in the Clinical Conditions section of the Abdomen.
Microscopic Anatomy
Just like the ureters, the urinary bladder consists of 3 layers: a mucosa/lamina propria, a muscularis, and an adventitia. The muscularis layer, more often called the detrusor muscle, is made up of very intertwined smooth muscle fibers. These fibers are arranged in an inner and outer longitudinal layer and an inner circular layer. When the detrusor muscle (de-tru’sor; “to thrust out”) contracts during urination, it squeezes the urine out of the bladder. In a state of emptiness the bladder collapses into its pyramidal shape and the inner mucosa forms folds, or rugae. As urine accumulates, the walls of the bladder stretch and the rugae flatten, allowing for adequate amounts of urine to be stored with a low pressure change. Because of the bladders great ability to stretch and distend, a full adult bladder can hold about 500ml of urine, which is 15 times the volume at empty.
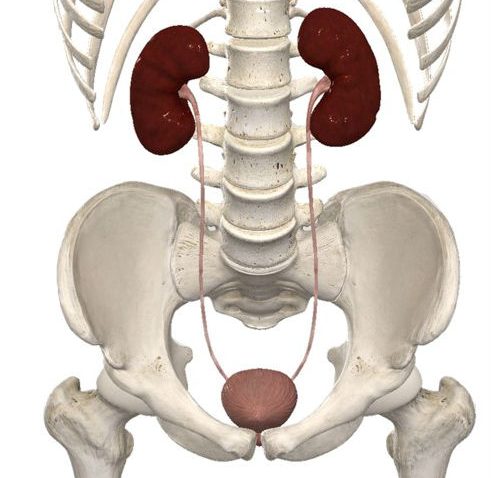
Figure 6.0. Image (with most internal organs removed) of the gross anatomy of the kidneys connecting to the urinary bladder via the ureters. Notice how the ureters exit the kidney through the hilum and enter the urinary bladder at an angle obliquely.
THE URETHRA
The function of the urethra as part of the urinary tract is to simply transport urine out of the body in women, and urine and semen out of the body in men. Micturition, which is also known as voiding or urination, is the process of emptying the bladder via the urethra. The urethra is a thinly lined lube consisting of an inner mucosa and smooth muscle. Where the bladder and urethra meet, the detrusor muscle thickens to form the internal urethral sphincter. The function of this sphincter is to keep the urethra closed when urine isn’t being passed through. The second, and last, sphincter of the urethra is called the external urethral sphincter. It is formed by a skeletal muscle called the urogenital diaphragm, and inhibits urination that isn’t voluntary. There are also some vast differences of the urethra in men and women. In women the urethra is very short (~3-4 cm) and opens at the external urethral orifice posterior to the clitoris. The very short urethra is a large reason why women are much more susceptible to urinary tract infections, as it is easier for bacteria to travel through the urethra to the bladder. In males, the urethra is roughly 5 times the length of a females (~20 cm) and is composed of three regions: the prostatic urethra, the membranous urethra, and the spongy urethra. The prostatic urethra runs through the prostate gland for about 2.5 cm and then transitions into the membranous urethra, which runs through the membrane-like urogenital diaphragm muscle for another 2.5 cm. The spongy urethra, the longest portion, is about 15 cm long and passes through the entire length of the penis where it opens at the tip via the external urethral orifice.
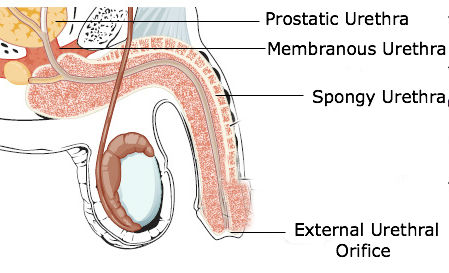 Figure 7.0. Illustration of a male urethra highlighting the 3 sections of the urethra: prostatic, membranous, and spongy.
Figure 7.0. Illustration of a male urethra highlighting the 3 sections of the urethra: prostatic, membranous, and spongy.
THE SPLEEN
The spleen is a secondary organ of the lymphatic system, where it filters blood and most importantly acts as the location of immune responses to blood-borne pathogens. The spleen is located in the upper right quadrant of the abdomen, it’s located under the rib cage and diaphragm.The roughly fist sized organ, which is the largest lymphoid organ, attaches to the lateral border of the stomach by means of the gastrosplenic ligament and is about 5 inches in length. Its concave anterior surface gives it a jellyfish like shape, curving around the left side of the stomach. The spleen it has two important ligaments; the gastrosplenic and the splenorenal ligaments. The outside of the spleen has two surfaces: gastric and renal. The splenic artery and vein enter the spleen through the hilum on the gastric surface. Its outer capsule consists of dense irregular connective tissue and some smooth muscle. The connective tissue capsule fibers form bundles, called trabeculae, which extend inside the spleen to divide it into multiple compartments. Inside each of these splenic compartments is an area of red pulp (mostly red blood cells) and an area of white pulp (similar to lymphoid follicles in a lymph node). The white pulp provides immune function to the spleen while the red pulp is responsible for the spleen’s ability to dispose of old and worn out blood cells. The white pulp consists of B and T lymphocytes surrounding the arteries of the spleen and the red pulp is made up of mostly splenic cords and venous sinuses. The spleen is also a storage center for blood platelets for life.
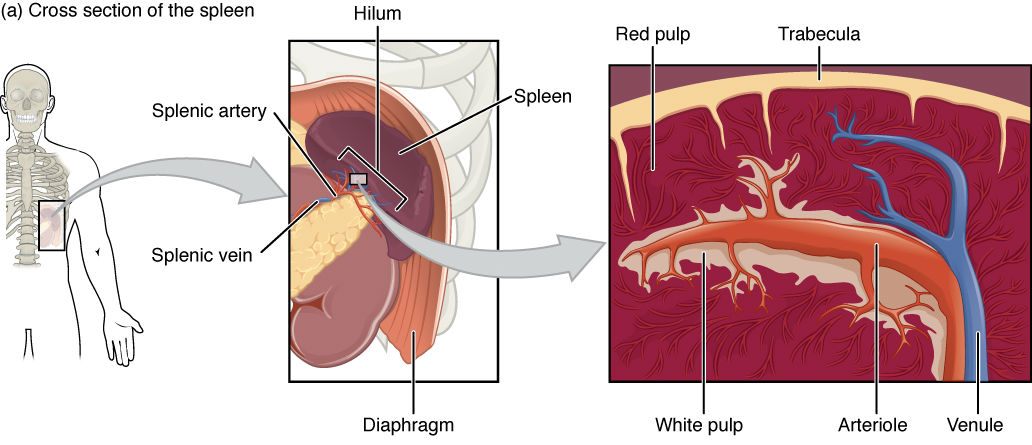
Figure 8.0. Cross section of the spleen showing the inner tissues separated into compartments by the trabeculae.
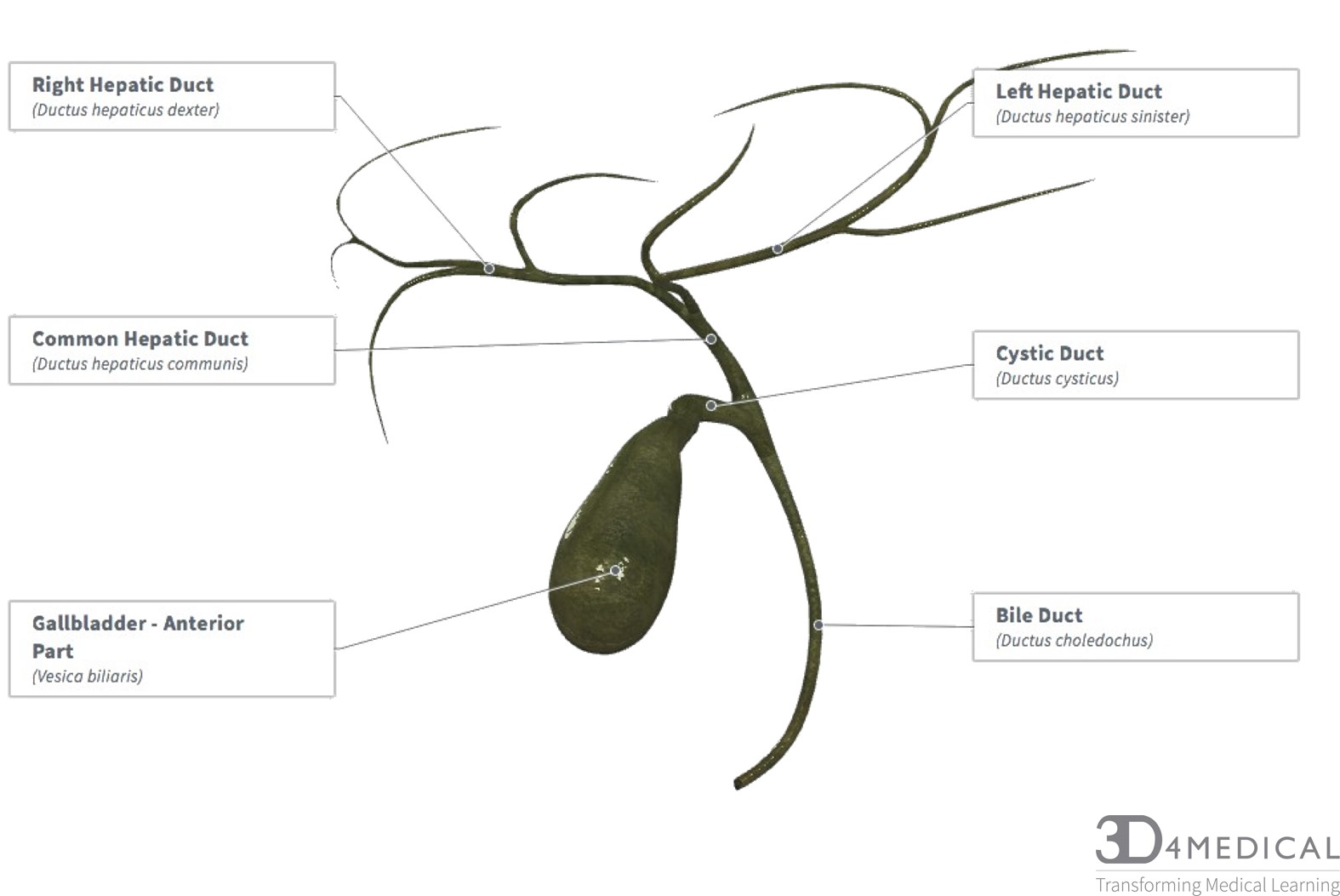
Gallbladder
This muscular sac is made up of the neck, body, and fundus. The gallbladder has many ducts attached to it. The cystic duct is the first duct coming out of the neck of the gallbladder, it joins with the common bile duct and common hepatic duct. The cystic duct has heister lining the walls which are mucosal folds, that helps move bile through the duct. The gallbladder can store 30-50 ml of bile at one time, and the parasympathetic nervous system contracts the gallbladder to release the bile into the biliary tree. The common duct is connected to the bile duct and two ducts from each lobe of the liver. The common hepatic duct takes the bile from the left and right lobe of the liver and delivers it to the duodenum through the common hepatic duct. The bile duct is connected by the common hepatic duct and the cystic duct. The bile duct empties into the pancreatic duct to empty bile into the pancreases. The gallbladders blood supply comes from the cystic artery and its vein is by the cystic vein, which drains into the portal vein. The nerve innervation for the sympathetic actions of the gallbladder is controlled by the coeliac plexus, the parasympathetic is controlled by the vagus nerve.
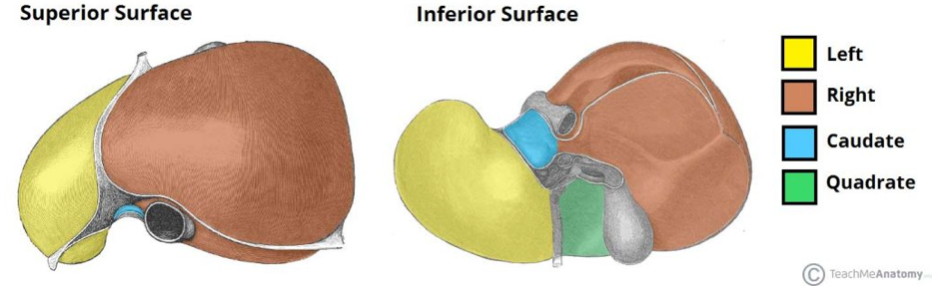
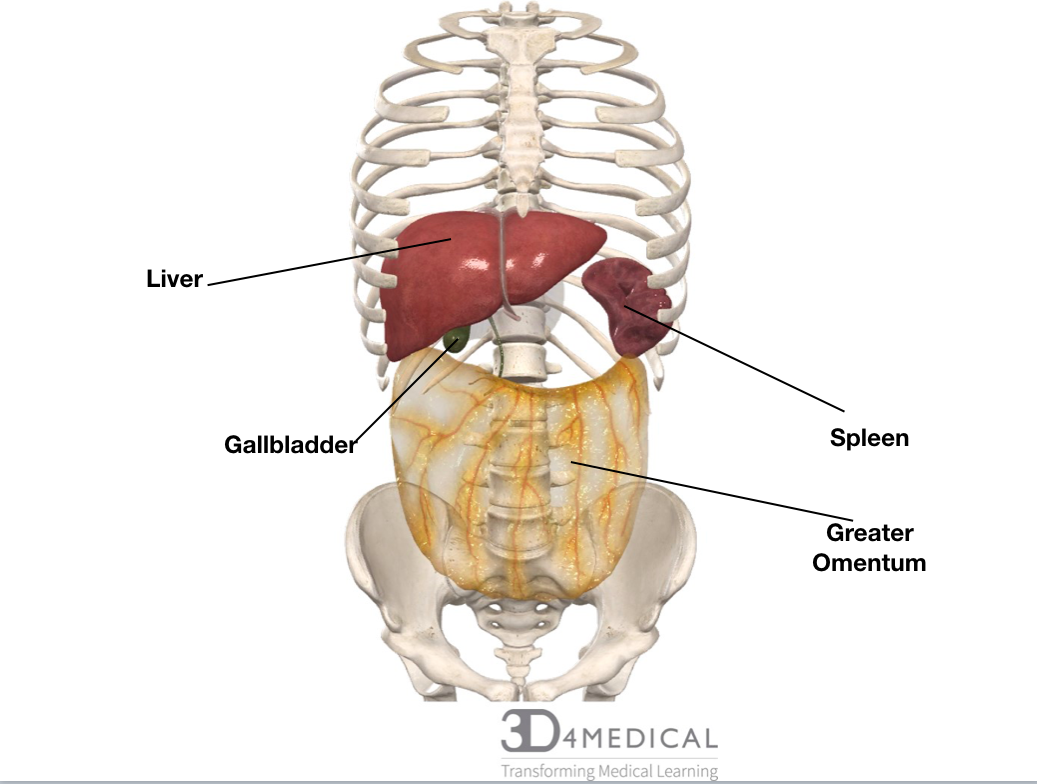
Liver
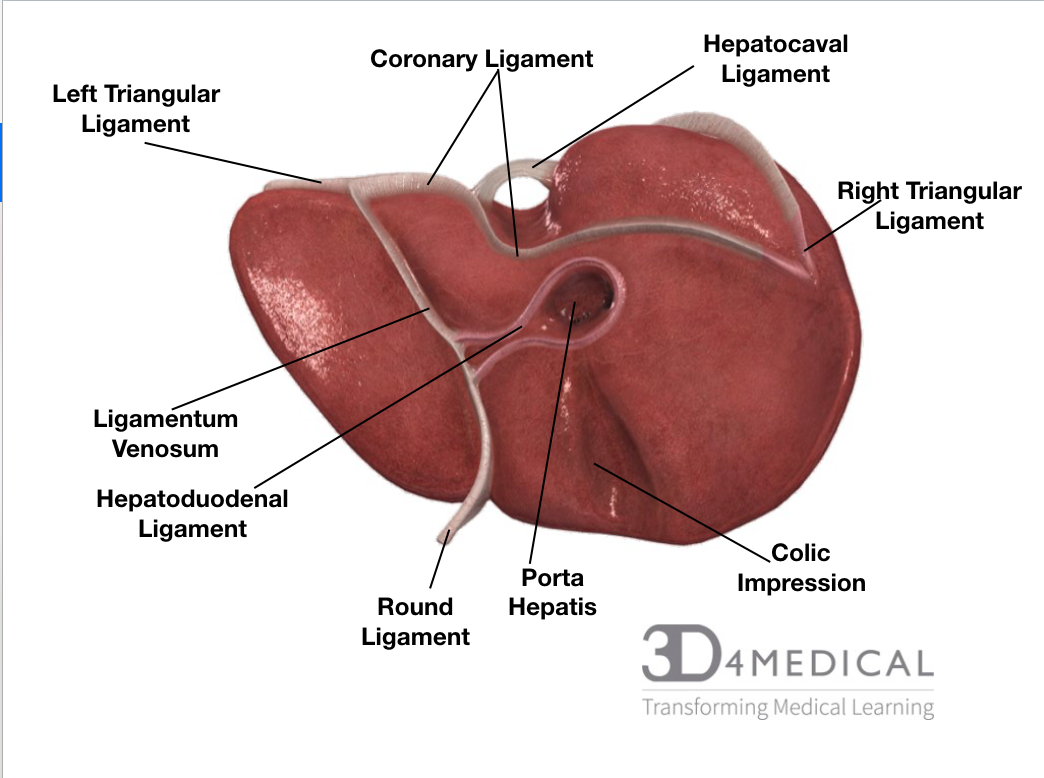
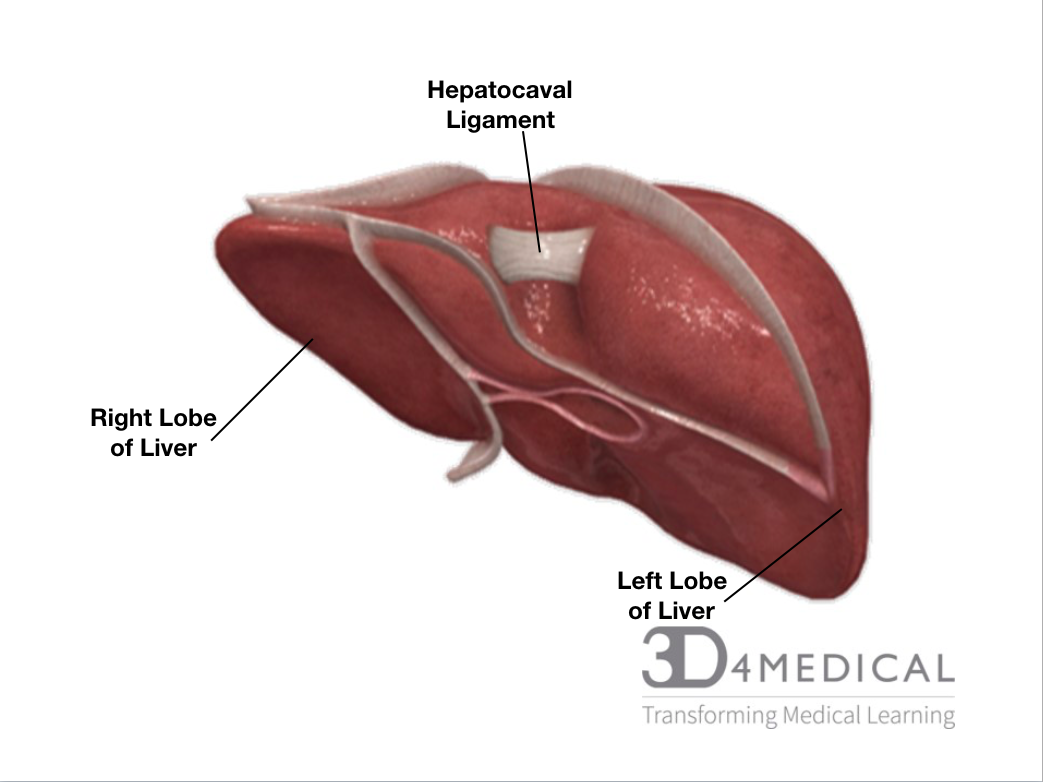
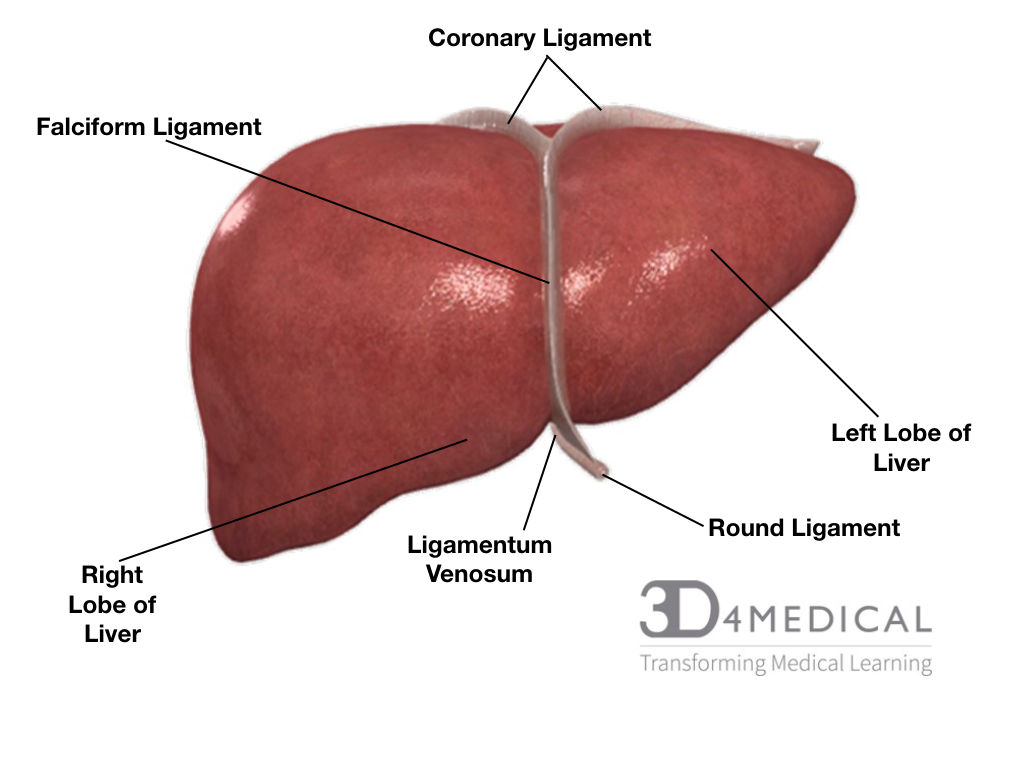
The liver is located in the right hypochondrium (the superior portion of the abdomen) and in epigastric areas. The liver has two different surfaces the visceral and the diaphragmatic. The diaphragmatic is the anterior superior surface of the liver, this portion touches the diaphragm and is sometimes referred to as the bare area, it curves outward and is very smooth. The visceral surface is the posterior inferior surface of the liver; this surface is covered with peritoneum excluding the porta hepatis. The peritoneum is a layer of connective tissue that lines most of the coelomic organs in the abdomen. The liver is split into four sections the left, the right lobe, the caudate lobe and the quadrate lobe; these lobes are divided by the falciform ligament. The porta hepatis is a deep fissure that divides the caudate and quadrate lobes. The liver has multiple ligaments, the falciform, coronary, and triangular (left and right). Along with many ligaments, the liver also has many spaces, subphrenic, subhepatic and Morison’s pouch. The blood supply for the liver comes from a branch of the hepatic artery, and the venues supply is a branch of the hepatic portal vein entering the liver. The liver’s blood supply system is quite unique, it has a dual blood supply with the hepatic arteries and the hepatic portal vein, this is called the hepatic portal system. The vein carries venous blood that has been taken from the spleen, gastrointestinal tract and its associated organs to the liver, hepatic veins carry blood out of the liver via the inferior vena cava. The system picks up nutrients and carries it to the liver for processing and storage. This system consists of two separate capillary bed lying between the arterial supply and venous drainage. The hepatic portal vein carries the deoxygenated blood that’s been cleaned by the liver. Related to the gallbladder the branch of the bile duct exits the liver. Innervation for the liver is supplied by the hepatic plexus, more specifically the fcoeliac plexus for sympathetic functions, and the vagus nerve for parasympathetic functions. Gilsson’s capsule, the layer of connective tissue surrounding the liver has its own separate innervation by the lower intercostal nerves. The liver has a specific cellular organization, hepatocytes, the cells of the liver are organized into lobules, the lobules are hexagon shaped with a central vein in the middle of each for draining. The hepatocytes carry out almost every function, each one has three periphery structures which are referred to as the portal triad. 500-1000ml of bile is produced a day by hepatocytes, the bile is a green alkaline liquid produced for digestive purposes. The hepatocytes have a rough endoplasmic reticulum for blood protein production, as well as a smooth endoplasmic reticulum helps with the production of bile salts and removes blood born poisons. An organelle in the liver called peroxisomes detoxifies other poisons such as alcohol. Sinusoids are a blood vessel found near the portal triads, they carry blood towards the central vein. Within the sinusoids, there are hepatic macrophages that fight against bacteria and other unwanted partials in the blood and removes old blood cells from the blood. Plasma is produced in mass amounts in the sinusoids to coat the hepatocytes.
Pancreas
The pancreas has two important functions, the exocrine and endocrine. For information on the endocrine functions of the pancreas go to the ventral organ section of the abdominal gland.
The pancreas’ exocrine functions as an important part of the digestive system. As 99% of the pancreas’ volume is dedicated to the exocrine function. The pancreas is responsible for producing digestive enzymes and buffers to be released into the duodenum. These are carried to the duodenum through the pancreatic ducts, more specifically the duct of Wirsung. There are also smaller accessory pancreatic ducts called Santorini ducts. At the Duodenal papilla, the common bile duct meets up with the pancreatic duct to be released into the duodenum.
The pancreas produces a wide variety of enzymes to finish the breakdown of the macronutrients before moving on into the rest of the small intestine, the ileum and jejunum, and colon where nutrient absorption occurs. The table below shows the enzymes released by the pancreas and each of the macronutrients it works on. The pancreas also releases bicarbonate which is a buffer that reduces the acidy of the acidic chyme that comes out of the stomach. A buffer is required to neutralize the acidy to prevent damaging the sensitive lining of the small intestine.
| Enzyme | What it breaks down |
| Pancreatic alpha-amylase | Carbohydrates to monosaccharides |
| Pancreatic lipase | Fats/lipids into fatty acids and glycerol with the help from bile from the gallbladder |
| Nuclease | RNA and DNA |
| Proteolytic enzyme (include Proteases, peptidase) | Proteins into amino acids |
Proteolytic enzymes make up about 70% of the all the pancreatic enzymes produced. This remains inactive until they are released into the small intestine. Examples of some specific proteolytic enzymes that are released by the pancreas include trypsinogen, chymotrypsinogen, procarboxypeptidase, and proelastase.
Video: https://www.youtube.com/watch?v=BtqlMr1rUT8
Greater Omentum
The greater omentum is referred to as the “protector of the abdomen”, it’s located at the greater curve of the stomach. It folds under itself and connects to the transverse colon. This organ is the largest peritoneal fold in the body, the fold is transparent and riddled with gastroepiploic arteries and drainage veins. This large tissue comes off the peritoneum and consists of fat, connective tissue, and portions of the lymphatic system. These lymphatic vessels aid in removing toxins and waste in this region. This great organ is divided into four different layers two anterior and two posteriors. The left side is a connection site for the gastrosplenic ligament and the right side is a connection site for the proximal duodenum. The main vessels that supply the greater omentum are the left, right and middle omental arteries. These arteries have smaller branches and drainage veins coming off them, the left and right artery supply the vascular system through an anastomosis. The greater omentum has seven important functions:
- The greater omentum deposits fats around various adipose tissue and this aids in keeping intestines warm.
- The lymphatic portion absorbs edema fluid in great amounts, which is a fluid that accumulates and causes swelling.
- Plays a role in support and protection of organs.
- Macrophage contained within protects against abdominal infections, the greater omentum can actually move to infected areas to send white blood cells to help fight off the infection.
- With its ability to move it can move to surround areas of trauma and isolate it from areas surrounding it to prevent further damage or spread of infection.
- Moves to sites of injury or infection to prevent drainage into the peritoneal cavity. (mostly appendix)
- Surgeons can use as graphing material.
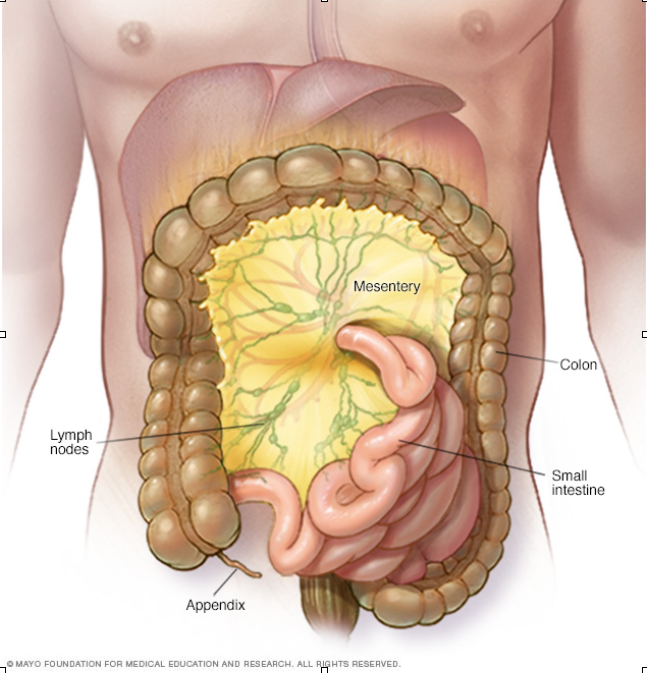
Mesentery
The mesentery surrounds many of the visceral organs in the abdominal region. Characteristics of the mesentery include two folds of peritoneal tissues holding the large and small intestines from touching the posterior side walls of the abdomen. This allows movement to occur, while still keeping all structures anchored it in place. The mesentery provides a space for blood vessels, nerves, and lymphatic vessels to run through. The mesentery is split up into different bending sections: the duodenojejunal, ileocaecal, hepatic, splenic and some in-between the descending portion and sigmoid colon, the sigmoid and rectum.
Intro to GI Tract
Overview of learning objectives:
After completing this section readers should be able to identify
> structures of digestive tract and key features
> layers of digestive tract organs including unique sections
> anatomical position of the organs of the digestive tract
> blood supply of digestive tract organs
> nerve innervation of digestive tract organs
You’ve probably heard the expression “trust your gut”, or “you are what you eat”. But does your gut really have a brain? Are you really made of food? Well yes… and no. Your “gut”, your gastrointestinal tract, your digestive system, alimentary canal, or whatever you want to call it is a complex system that takes complex substances (food) and breaks them down into less complex parts (nutrients and minerals) that are essential to maintain bodily functions, and life as we know it. Everyday your body regenerates upwards of 50 billion cells, and it needs nutrition to promote that regeneration – meaning that your body uses the essential nutrients and minerals from food to rebuild it’s own cells. The enteric nervous system innervates the entire digestive tract. This involves a very specific monitoring process, thus your digestive tract relies on a vast network of nerve plexus’ to relay information, and maintain homeostasis – these nerve plexus live in the layers of your digestive tract. They are essentially the “brain in your gut”.
The digestive system has the vital responsibility of breaking food down and converting it into nutrients and energy to nourish and sustain the body. It is made up of organs and accessory organs that all play a critical role in this process. This section will cover the anatomical features of the system and core structures that food travels through during the digestive process. The GI tract starts at the mouth, but for organizational purposes, this section begins at the esophagus and ends with the large intestine. These regions are depicted in figure 1. Blood supply and nerve innervation will also be covered. The gut is innervated by the enteric nervous system; the enteric nervous systems is distributed throughout the walls of the gut. It’s main function is to initiate peristalsis (muscle contractions that pass bolus/chyme through the tract) and trigger the release of digestive hormones. The plexus responsible for peristalsis is called “Auerbach’s plexus” and it is located between the muscular layers. Additionally, the Meissner’s plexus lies in the submucosa, it’s role is control of secretions and blood flow. Parasympathetic and sympathetic impulses also trigger nerves to inhibit or promote activity. They are influenced by other sensory nerve endings located in the epithelial lining.
Figure 1. Organs of the digestive system.
Picture the human body as a giant tube, and the alimentary canal is the hole in the middle. Food travels through the tube “outside of the body” in the lumen, during this process the body extracts what it needs, and disposes of what it doesn’t. The external layer is the interface between the GI tract and surrounding tissue, it is referred to as either the adventitia or the serosa, depending on its location in reference to the peritoneum (serous membrane of abdominal cavity). A common theme of anatomy is “form fits function”; each of the passageways has a unique structure with implications for the type of digestion, mechanical or chemical, and specific to the absorption that occurs at each site. In general, the GI tract has 4 distinct layers; the mucosa, submucosa, muscular and serosa. While these layers are common to each section, each organ has unique features with diverse functional implications, table 1 summarizes these differences. For anatomical reference, this text refers to the 9 divisions of the abdomen as shown in figure 2.
Table 1. Summary of the 4 layers of the gastro-intestinal tract, highlighting region specific features.
|
mucosa |
submucosa | muscularis externa | adventitia (adhered)
/ serosa (suspended) |
|
|
esophagus
|
|
elastic fibers |
A |
|
|
stomach |
|
gastric rugae |
oblique layer |
S |
|
small intestine:
|
|
|
|
|
|
large intestine:
|
|
taenia coli |
|
|
| appendix | see large intestine | lymphoid nodules | no taenia coli |
S |
Esophagus
Structure and key features
The Esophagus, sometimes referred to as the Oesophagus, is the 25cm muscular tube that connects the pharynx (throat) to the stomach. It is described in 3 parts, Cervical (4cm), Thoracic (20cm), and Abdominal (12cm). The superior opening of the esophagus is surrounded by a group of skeletal muscles called the upper esophageal sphincter or UES. The Cricopharyngeus is the main muscle responsible for the closing of the esophagus which is a vital function of the structure as it ensures that food doesn’t re-enter the pharynx.
Peristalsis is the process of moving food along the digestive tract, it is the result of a series of circular and longitudinal muscular contractions. No digestion occurs in the esophagus – it is simply responsible for moving food from the mouth to the stomach.
At the inferior end of the esophagus is the lower esophageal sphincter or LES. It is classified as a physiological sphincter, lacking specific muscles. It is located at the gastroesophageal junction. This opening allows food into the stomach, and when functioning correctly, closes to prevent the acidic liquids of the stomach from travelling back up. If these muscles are weakened, acid reflux can occur; the acidic contents of the stomach enter the upper digestive tract which can damage the esophageal lining. This type of damage can potentially lead to complications such as esophageal cancer if not treated.
Layers
As previously suggested, the digestive tract is comprised of 4 functionally significant tissue layers; the mucosa, submucosa, muscularis, and adventitia. The esophagus is unique as it contains a mixture of skeletal and smooth muscle. These layers are summarized in table 1.
Anatomical position
The esophagus lies posteriorly to the trachea, and is continuous with the laryngeal part of the pharynx. It extends from the lower border of cricoid cartilage of the larynx at C6, penetrates the abdomen via the esophageal hiatus, descending into the superior mediastinum of the thorax at T10, and enters the cardiac orifice of the stomach at T11. The junction is marked by a transition of stratified squamous epithelium of the esophageal mucosa, to the simple columnar epithelium of the gastric mucosa. The phrenoesophageal ligament – bit of a mouthful, but “phreno” relates to the diaphragm, and “esophageal” relates to the esophagus – connects the esophagus to the border of the hiatus (opening) in the diaphragm, which permits independent movement of the two appendages.
Blood supply
The cervical portion of the oesophagus is supplied by the inferior thyroid arteries. Blood is supplied to the thoracic region via the esophageal branches of the descending thoracic aorta and bronchial arteries. Lastly, the abdominal part is supplied by the esophageal branches of the left gastric and phrenic arteries.
Nerve innervation
The motor and sensory functions here are controlled by branches of the glossopharyngeal and vagus nerves. The sympathetic fibres originating from T5-T9 spinal segments are sensory and vasomotor.
Stomach
Structure and key features
The stomach is a crescent shaped, receptacle organ that stores food between the esophagus and intestines. It is commonly divided into four regions differing based on the shape and actions (form fits function!). The narrow transition from the esophagus is called the cardia. Within the cardia is the lower esophageal sphincter. The cardia empties into the body, the central and largest region of the stomach. The stomach also bulges superiorly creating the fundus, where gases released through chemical digestion are stored. The inferior section of the stomach is the pylorus, where the pyloric sphincter controls the flow of chyme (partially digested food) between the stomach and the duodenum.
As mentioned previously, the transition from the esophagus to the stomach is observable via the change in the epithelial composition. The junction is marked by a transition of stratified squamous epithelium of the esophageal mucosa, to the simple columnar epithelium of the gastric mucosa. The differing epithelial layers, are associated with different functional requirements (re: form fits function!).
The size and position of the stomach varies greatly among body types, weight, volume, fluid / food content, body posture and respiration.
Layers
As previously stated, the digestive tract is comprised of functionally significant tissue layers. A unique feature of the stomach is that it has three complete muscular layers – longitudinal, circular and oblique – that allow for the churning motion. However, similar to the other sections of the digestive tract, the stomach is comprised of 4 layers; the mucosa, submucosa, muscularis, and adventitia. Each region of the stomach has a unique composition of mucosal glands.The layers of the stomach are summarized in table 1.
Anatomical position
The stomach changes orientation and position in relation to respiration, content, and bodily posture. This text will consider the stomach from a supine position, dividing the abdominal region into 9 quadrants (see figure 2). From this perspective, the cardia and fundus sit posteriorly to the costal cartilage of the 6th rib. The pylorus sits above and below the junction of the epigastric and umbilical regions. The greater curvature extends from the 5th intercostal space down to the hypochondrium, entering the upper middle part of the left lateral flank and meets the pylorus in the umbilical region. The lesser curvature extends from the cardia to the uppermost aspect of the pylorus at a junction called the angular notch.
Blood supply
The most superior portion of the greater curvature and the fundus (see figure 3) are supplied by the short gastric arteries, branches of the splenic artery. The inferior part is supplied by the right gastric artery, a branch of the hepatic artery which branches from the common hepatic artery.
Nerve innervation
The stomach receives innervation via multiple sources. The vagus nerve is responsible for parasympathetic (the “rest and digest” system) supply to the stomach, it enters the abdomen through the esophageal hiatus in the diaphragm. The anterior vagal trunk supplies the front of the stomach, and the posterior part of the stomach is supplied by the (you guessed it) posterior vagal trunk. The sympathetic nerve supply (the “fight or flight” system) is contributed by the celiac plexus which receives fibers from T6 – T9, via the greater splanchnic nerve.
Clinical significance
Anti-inflammatory drugs prescribed to fight arthritis, can cause stomach or peptic ulcers; which are sores that develop in the lining of the stomach and small intestine. Ulcers occur when the stomach’s protective layer is broken down and the corrosive stomach acid damages the lining. Non-Steroidal Anti-Inflammatory drugs (NSAID’s) which are prescribed to treat inflammation, commonly arthritis, can inhibit production of the stomachs protective lining. Such drugs have a topical irritant effect on epithelium, they impair the barrier properties of the mucosa, suppress gastric prostaglandin synthesis (lipid compounds that promote tissue regeneration, but are inflammatory in nature) and reduce gastric mucosal blood flow which is essential for repairing the damage. Basically they interrupt the process of protecting the stomach lining from the acidic liquids that are essential for breaking down food.
When food is broken down according to plan, via chemical digestion in the stomach, it is ready to enter the small intestine.
Small Intestine
Structure and key features
The stomach transitions to the small intestine via the pyloric sphincter – the first segment that the chyme (partially digested food) passes through is called the duodenum. The small intestine, or small bowel, is divided into 3 parts; the duodenum, the jejunum, and the ileum (not to be confused with ilium). The small intestine is the longest organ in the body, measuring over 3 meters long. It’s length and the presence of plicae circulares and villi lined walls contribute to its immense surface area (over 100x that of the skin!) enabling it to be the primary location for digestion and absorption (Re: form fits function). It is called the “small intestine” in reference to its narrow diameter, 2.5 cm compared to the 7.6 cm opening of the large intestine. The small intestine spans from the pylorus to the ileocaecal junction.
Layers
As previously suggested, the digestive tract is comprised of functionally significant tissue layers. The small intestine is made up of 4 layers; the mucosa, submucosa, muscularis, and adventitia. The mucosa of the small intestine has 3 unique features that increase its surface area thus, improving it’s absorptive and digestive abilities. These features are plicae circulares (circular folds), villi (finger like projections) and microvilli (smaller finger like projections / striated border of the villi). The rest of the 4 layers are summarized in table 1.
Anatomical position
The small intestine is divided into three anatomical sections; the duodenum, the jejunum, and the ileum. The proximal portion, the duodenum, is the shortest, 5 cm in length and shaped like a “C”. It begins at the pyloric sphincter and is considered retroperitoneal (it runs posteriorly to the peritoneum). The duodenum runs from the pylorus to the duodenojejunal junction and is divided into four parts; superior, descending, inferior and ascending. The superior section is 5cm long, it ascends upwards from the pylorus at L1, it is connected to the liver. The descending portion curves inferiorly from L1 to L3, around the head of pancreas. The inferior duodenum travels laterally to the left at L3, crossing the inferior vena cava and aorta. It is inferior to the pancreas and posterior to the superior mesenteric artery and vein. The ascending portion crosses the aorta, and curves anteriorly to join the jejunum at the duodenojejunal flexure at around L2. At this flexure the intestine transitions from being retroperitoneal to intraperitoneal. The jejunum measures around 0.9 meters long. Lastly, the ileum runs along the right side of the abdominopelvic cavity in the umbilical and hypogastric regions – it is roughly 3-4 cm long, and it transitions to the colon via the ileocecal sphincter.
Blood supply
The main artery that supplies the small intestine is the superior mesenteric artery that branches from the abdominal aorta, inferior to the celiac trunk. It also provides oxygenated blood to the proximal large intestine. It forms five major branches including the inferior pancreaticoduodenal artery, which supplies blood to the distal end of the duodenum. Next the intestinal arteries that feed the tissues of the jejunum and ileum form a network of arteries to prevent interruptions to blood flow to the intestine. The ileocolic artery, provides blood to the terminal ileum, cecum and appendix. Nutrient rich blood blood from the intestine is carried to the liver via the hepatic portal vein.
Nerve innervation
The small intestine receives both sympathetic and parasympathetic innervation. The sympathetic supply originates from T10 and T11 sections of the splanchnic nerves and superior mesenteric plexus. The vagus nerve provides parasympathetic fibers via the celiac and superior mesenteric plexuses. The superior mesenteric artery supplies the whole small intestine and extends to the middle third of the transverse colon before the vagus nerve takes over. Sympathetic fibres play a role in the motor function of the intestinal sphincters, the parasympathetic fibres stimulate peristalsis and inhibit said sphincters.
Clinical Relevance
Crohn’s and colitis can take many forms, the most common is inflammatory bowel disease, or “ileocolitis”, so named as it affects both the ileum and the colon. It is a chronic condition whose cause is relatively uncertain, but is thought to be linked to genetics or caused by stress or malnutrition. Ileiocolitis is an autoimmune disorder, it causes damage to the intestinal walls and inhibits its ability to absorb essential nutrients. The inflammation causes a defensive response that attacks healthy cells, preventing the cell walls from regenerating properly, and causing a thickening of the intestinal wall as it is in a constant state of repair. These circumstances cause swelling, abdominal pain, diarrhea, digestive complications and potentially lead to fistulas and ulcers. It is not inherently life threatening, but failing to treat symptoms or make healthy changes can potentially lead to cancer and other complications.
Treatment is available for Chron’s disease although there is no cure. Healthy diet changes, antibiotics, prescription medicines, herbal remedies, and surgery are all options for reducing and managing symptoms.
Large Intestine
Structure and key features
Because of their close relationship, diseases like Crohn’s/Colitis can affect both the small and large intestine. However, there are structural differences between the two intestinal tracts. The small intestine turns into the large intestine at the ileocecal valve. The large intestine is shorter, but gets its reputation form it’s much larger diameter. It is also distinguished by the presence of omental appendices, haustra, and teniae coli. It’s tissue layer is common to that of the appendix and the rectum and, the large intestine is often referred to as the colon. The large intestine can be divided into 5 sections; the cecum, appendix, colon, rectum and anal canal. It measures approximately 1.5 m in length, about half the length of the small intestine. The colon is further subdivided into the ascending, transverse, descending and sigmoid colon.
Layers
Unlike the small intestine, the colon lacks villi. It’s simple columnar epithelium, does however, contain several goblet cells. Additionally the presence of teniae coli, found just deep to the serosa, differentiate the large from the small intestine. Teniae coli are three incomplete layers of longitudinal smooth muscle tissue covering the ascending, transverse, and descending colon. The other tissue layers of the large intestine are summarized in table 1.
Anatomical position
The large intestine starts in the right iliac region of the pelvis, below the right waist. It makes up about one-fifth of the length of intestinal canal. The ileum opens to the cecum via the ileocecal sphincter on the medial side, the cecum is the proximal section of the large intestine. The cecum is continuous with the ascending colon, it runs superiorly on the right side of the abdomen from the right iliac fossa to the right lobe of the liver. At the right colic, or hepatic, flexure, the colon turns left. The transverse colon is the largest section of the large intestine. It is located between the right and left colic flexure. The transverse colon transitions to the descending colon (between the left colic flexure superiorly, and inferiorly to the left iliac fossa) and then finally to the sigmoid colon. The sigmoid colon is the link between the descending colon and rectum, it is S-shaped (hence “sigmoid”) and turns into the rectum at the third sacral vertebrae.
Blood supply
The superior and inferior mesenteric arteries provide bloody supply to the colon. Intra-arterial communication occurs via the marginal artery. There are specific branches that supply specific portions of the bowel, for example, the cecum is supplied by the ileocolic artery. Additionally, this branch supplies the appendix via the appendicular artery. The ascending colon is supplied through the right colic artery. The transverse colon receives blood from the middle colic artery. The descending and sigmoid colon both receive oxygenated blood via the left colic, and sigmoid arteries. Lastly, the rectum and anal canal receive blood from the inferior mesenteric artery.
Nerve innervation
The ascending and proximal two-thirds of the transverse colon, receive parasympathetic, sympathetic, and sensory nerve innervation via the superior mesenteric plexus. The distal third of the transverse colon, descending colon and sigmoid colon receive parasympathetic, sympathetic and sensory nerve innervation from the inferior mesenteric plexus. The inner circular and outer longitudinal smooth muscles play host to a number of Auerbach’s plexus scattered in between.
